Complex Reconstruction at Stanford

Multiple fixation techniques were used to reconstruct metacarpal fractures.
Patients may require reconstructive surgery after severe trauma, birth problems, or cancer. Optimal reconstruction may involve multiple staged procedures, new biomaterials, and/or microsurgical transplants.
At Stanford, Complex Reconstruction patient's needs are unique. Therefore, the surgical plan must be individualized.
Clinical care is coordinated with specialties such as Radiology, General Surgery, Oncology, Orthopedics, Otolaryngology, and Vascular Surgery.
Innovative Techniques
The development and use of new techniques, as well as creatively employing traditional methods, allows state-of-the-art reconstruction to restore optimal form and function.
- Microvascular surgery
- 3D CT angiography for pre-operative planning
- Peripheral nerve surgery with intra-operative nerve monitoring
- Endoscopic guidance for fracture reduction
- Resorbable plate fixation
- New bone and skin biomaterials
- Distraction osteogenesis
- Perforator flaps (anterolateral thigh [ALT], deep inferior epigastric perforator [DIEP] flap)
- Continuous post-operative monitoring.
Complex Reconstructive Problems Addressed
- Emergency hand and limb replantation
- Complex wounds requiring flap surgery
- Exposed orthopedic hardware
- Industrial accidents
- Lower limb salvage
- Wrist and hand fractures
- Facial fractures
- Complex jaw surgery
- Immediate breast cancer reconstruction
- Delayed breast cancer reconstruction
- Peripheral nerve injuries
- Exposed bone or tendon
- Brachial plexus injuries
- Avascular necrosis of wrist bones
- Radiation damage
- Melanoma reconstruction
- Hand and neck cancer reconstruction
- Foot drop
- Flexor tendon reconstruction
- Tendon transfers
- Chest wall reconstruction
- Sternal wound infections
- Facial paralysis
- Thumb reconstruction (toe-to-thumb transfers)
- Abdominal wall reconstruction
- Delayed burn reconstruction
- Scalp reconstruction
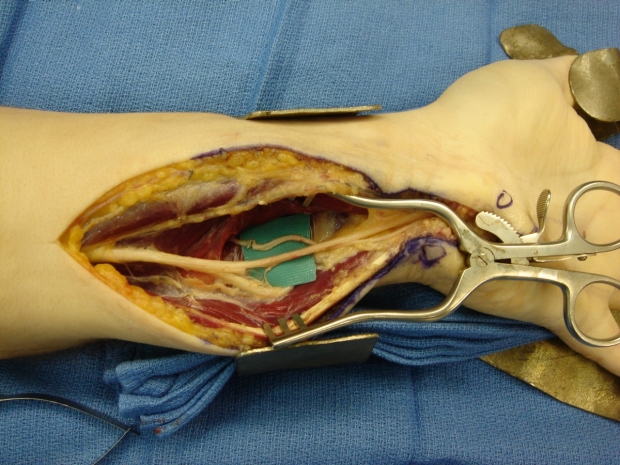
The anterior interosseous nerve was transferred to the motor branch of the ulnar nerve in order to more rapidly restore hand muscle function.
For appointments and to learn more about this option, please visit Making an Appointment or contact our Plastic Surgery Clinic at (650) 723-7001.

TRANSFER INFORMATION
Each patient referred to the Center will undergo a comprehensive evaluation, and a reconstructive plan will be determined before surgical reconstruction is performed. The goal is to restore best possible form and function to return patients to their normal daily activities.
Emergency Department Transfers
Physician consultation, transfer of trauma patients and other patients with emergency medical conditions are facilitated 24 hours a day.
Hospital Inpatients
Inpatients requiring consultation or higher level of care for complex reconstruction are faciliated through the Stanford Transfer Center.
Emergency and Inpatient:
1-800-800-1551 or (650) 723-4696
Clinic Outpatients
Requests for consultations or clinic appointments are facilitated through the Stanford Referral Center (1-866-742-4811).

This post-operative 3D CT angiogram showed patent vessels and good bone alignment after the fibula bone was transplanted to reconstruct the maxilla in the face.